Today we discussed a case of a patient with jaundice from decompensated cirrhosis with encephalopathy, hepatorenal syndrome, and likely spontaneous bacterial peritonitis, who had a decreased level of consciousness.
The presumed etiology was ETOH cirrhosis with possible co-morbid hemochromotosis (NEJM review and recent study). Hemochromotosis is suggested when the transferrin saturation is above 45% (NB: in liver failure the transferrin levels may be low, artificially increasing the iron saturation) and/or the ferritin is above 200 in women and 300 in men.
There is a complex interplay between ETOH and iron overload with the two compounding to cause liver dysfunction as suggested in this article.
We also briefly noted the association between increased IgA and alcoholic liver disease.
He also had a traumatic subdural hematoma which needed to be urgently decompressed.
Wednesday, May 13, 2009
Tuesday, May 12, 2009
Day #306 - TB Pleuritis

We discussed a great case of tuberculosis causing pleural effusion today. I have previously blogged about this before.
Previous blogs on pleural effusion here and here (including discussion of Light's Criteria and parapneumonic effusions/empyema).
Modified Light's Criteria (see review here):
- Change LDH pleural fluid 0.45 ULN (increases sensitivity but reduces specificity)
Alternative tests:
- LDH (0.45ULN), cholesterol (45mg/dl) and protein (29g/L) of pleural fluid, done in combination have similar performance characteristics to Light's criteria and don't require paired serum samples.
Monday, May 11, 2009
Day #305 - HIV Lymphoma
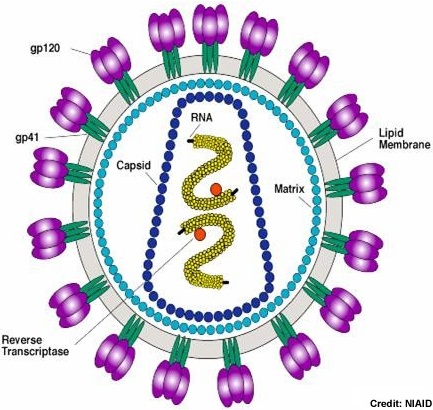
Today we discussed a case of a patient with known HIV disease (CD4 300-500, not on therapy) who presented with fever, diffuse adenopathy, and splenomegaly. The presumed cause is lymphoma.
The differential diagnosis would include:
Infections:
- HIV with high level viremia
- Mononucleosis syndromes (EBV, CMV, acute toxoplasmosis)
- Syphilis
- Disseminated TB
- In the more immunosuppressed host:
- Mycobacterium Avium Complex
- Bartonella Henselae
- Disseminated fungal infection (i.e. histoplasmosis)
- Non-infectious
- Lymphoma
- Multicentric Castleman's Disease
- Sarcoidosis
- Lymphoma
I have previously blogged about HIV here, here (with cryptococcal meningitis), and here (with PCP pneumonia).
I have blogged about lymphoma including staging here.
A review of the pathology of HIV associate lymphomas is here. An article reviewing the treatment of HIV associated lymphoma is here.
Friday, May 8, 2009
Scenario Rounds - Wolff Parkinson White Syndrome


What to do with symptomatic patients? (ACC Guidelines on ablation, ACC Guidelines on the management of supraventricular tachycardia)
AVRT is the most common arrythmia seen in WPW.
- If you've had sudden death -- you need an ablation.
- If your refractory period is short (less than 240ms) you should consider an ablation to prevent sudden death.
- Risk of cardiac death is about 0.25% per year or 3-4% over lifetime, with the majority of the risk in patients with refractory periods of the accessory pathway that are less than 220ms.
- Success of ablatation approaches 95% with ~ 5% recurrance rate.
- Risk of major complications is ~ 2% including:
- complete heart block 0.2-1%
- tamponade 0.3-1%
- stroke 0.2-0.5%
- death 1-2 per 1000.

- Risk of major complications is ~ 2% including:

What to do with asymptomatic patients with WPW on ECG?
Low risk for sudden death is seen in patients who lose the conduction via the accessory pathway during exercise (or stress), patients with intermittant pre-excitation (comes and goes), and patients who stop conducting down the accessory pathway when given a dose of procainamide. Low risk patients should receive a copy of their ECG with diagnosis and should be managed expectantly.
Patients without low risk features should be considered for EP study, and if high risk features on EP study are found should be considered for ablation, depending on age, gender, occupation, athletic lifestyle.
NB: One of the earlier publications, by Wolff, is available here.
Thursday, May 7, 2009
Day #301 - Pheochromocytoma

Today we discussed the case of a patient with the classic presentation of paroxysms of hypertension, headache (80%), palpitations (60%), and diophoresis (70%).
This is a rare diagnosis occuring in approximately 1-2 per 100,000. Approximately 10% will be extra-adrenal. About 10% of sporatic pheo will be malignant. Approximately 10% will have metastasis.
25% of patients may have a genetic predisposition to pheochromocytoma. Syndromes which include a propensity to pheochromocytoma include neurofibromatosis type 1, von hippel lindau, Multiple endocrine neoplasia types 1 and 2
A review of the condition and the diagnostic algorithm is available here.
Initially control of the BP should be achieved with alpha blockade, with agents like phenoxybenzamine (10 mg PO BID titrated every 2-3 days by 10-20mg until achieving effect), prazosin or terazosin. For long term use, prazosin or terazosin are theoretically preferred to phenoxybenzamine b/c of shorter half lives and fewer side-effects. They should be started 7-10 days pre-resection.
Beta-blockers are then added to control tachycardia and arrythmias -- but only after alpha blockade has been achieved.
Calcium channel blockers may safely be used as an adjunct for hypertension.
The goal SBP is 120 lying or sitting.
Pre-op patients should receive intravenous crystalloid to achieve a good ECF volume. This will help avoid post operative hypotension. The preferred operative route is to perform a laparascopic resection of the adrenal mass.
Catecholamine levels should return to normal by 10 days post op. Failure to decrease suggests a residual PHEO.
Post resection patients should be followed periodically for recurrence.
Tuesday, May 5, 2009
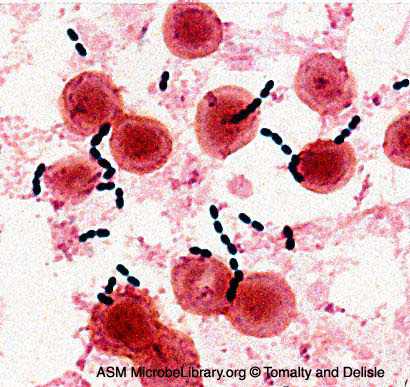
Day #299 - Enterococcal Prosthetic Valve Endocarditis
Great case. I have previously blogged about the diagnosis of endocarditis here and here.
Patient with multiple prosthetic valves develops sepsis in the context of an enterococcal bacteremia. Highly suspicious though non diagnostic echo for PVIE. Treated with VANCOMYCIN ("penicillin allergy" is a pet peeve of mine) and GENTAMICIN (for synergy). The evidence for synergy is not totally supported by clinical experience. Nephrotoxiciy is common but similarly has not been shown to impact mortality. The combination of VANCOMYCIN with an aminoglycoide increases the risk of nephrotoxicity.
We also reviewed aminoglycoside ototoxicity -- presenting either as sensory-neuro hearing loss or vestibulary dysfunction.
This patient developed renal failure presumably related to ATN from the VANCO+GENT; however, one can get a glomerulonephritis in endocarditis.
There is evidence that AMPICILLIN plus CEFTRIAXONE (which usually has no enterococcal coverage) can be used effectively in the treatment of enterococcal endocarditis.
Patient with multiple prosthetic valves develops sepsis in the context of an enterococcal bacteremia. Highly suspicious though non diagnostic echo for PVIE. Treated with VANCOMYCIN ("penicillin allergy" is a pet peeve of mine) and GENTAMICIN (for synergy). The evidence for synergy is not totally supported by clinical experience. Nephrotoxiciy is common but similarly has not been shown to impact mortality. The combination of VANCOMYCIN with an aminoglycoide increases the risk of nephrotoxicity.
We also reviewed aminoglycoside ototoxicity -- presenting either as sensory-neuro hearing loss or vestibulary dysfunction.
This patient developed renal failure presumably related to ATN from the VANCO+GENT; however, one can get a glomerulonephritis in endocarditis.
There is evidence that AMPICILLIN plus CEFTRIAXONE (which usually has no enterococcal coverage) can be used effectively in the treatment of enterococcal endocarditis.
Friday, May 1, 2009
Day #295 - Tuberculosis and Immune Reconstitiution

We discussed a case of pulmonary and extrapulmonary tuberculosis which presented on TNF-alpha antagonist therapy.
Addendum: TB Immune Reconstitution Reviewed Recently here.
We also discussed paradoxical worsening of TB post-discontinuation of immunosuppression. The case report I was talking about is available here.
Subscribe to:
Posts (Atom)